28 November 2014With over 35 million victims since its explosion in the 1980s, and as many individuals currently living with it, HIV/AIDS has duly acquired a status of exception in the popular imagination on public health. It is, indeed, the most aggressive epidemic of our recent history. The creation of the World AIDS Day, in 1988, seemed to mark the turning point of a permanent collaboration between governmental structures, independent bodies and individual initiatives towards the ideal of an hygienic world. But have we settled this yearly celebration for the lower goal of an awareness effort, when the actual objective should indeed be the total eradication of the virus? Then, what are really the scopes of concerted efforts, when deep shifts within and across cultures have not been attempted radically? Where sex is a familial taboo, children can, rightly, only turn to the education system to get the exposition guaranteeing at once the blossoming of each and the safety of all. And schools will be at the forefront of the national campaigns of awareness raising, this December 1st. But how far can these singular programmes percolate down into an education culture still gravely curbed by the puritanism of Victorian values? Indeed, AIDS is more than a disease: it has become an episode in the cultural history of humanity, and only a thorough cultural response will succeed in making the current generation the last HIV-positive humans of history, and thus closing its legacy. So that we are not observing the World AIDS Day on the 1st December in ten, fifty or hundred years. This week on LILA Inter-actions, Glory Alexander looks back at 28 years of responses to HIV/AIDS in India; she singles out the successes and remains concerned about the deep cultural hindrances. Rajesh Talwar evaluates the authenticity of world political leaders around the cause, and he explains how he discovered literature, and in particular theatre, as a powerful means to energise and complement institutional initiatives. Hold the cursor on the illustrations to display animations. |
|||||||||
Prevention, Care and SupportGlory Alexander |
Creating SolutionsRajesh Talwar |
||||||||
Error occurred when trying to fetch the file using wp_remote_get(). stream_socket_client(): php_network_getaddresses: getaddrinfo failed: Name or service not known
stream_socket_client(): unable to connect to ssl://dl.dropbosxusercontent.com:443 (php_network_getaddresses: getaddrinfo failed: Name or service not known) |
Listen |
Listen |
Error occurred when trying to fetch the file using wp_remote_get(). stream_socket_client(): php_network_getaddresses: getaddrinfo failed: Name or service not known
stream_socket_client(): unable to connect to ssl://dl.dropboxuserscontent.com:443 (php_network_getaddresses: getaddrinfo failed: Name or service not known) |
||||||
|
HIV/AIDS has gone a long way since its entry in India in 1986. Its public recognition, and the responses in terms of therapy and counselling have largely improved. But a number of issues are still topical today. Stigma and discrimination (S&D), to start with, as well as the societal exclusion of those who are HIV-positive, remain hindrances to the fight against HIV/AIDS. Stigma and discrimination exist in the family, in the community, in the schools, in the workplace, in the medical setting and in the media. However, at the macro level, S&D have improved considerably. There used to be a time when media messages and hoardings would instil fear. They were of a warning nature and the focus was on sensationalism. Now, the media is more sensitive and understanding. Heart-warming stories are written on HIV-positive women who have overcome all the obstacles and sorrows in their lives to create a positive environment around themselves and their children.  On the TV reports about AIDS, the tone has changed
In the medical setting too, there are now many hospitals caring for PLHIV (Persons Living with HIV) and they deliver positive pregnant women. The Government, also, has started free ART centres (Anti Retroviral Therapy), and there are around 425 ART centres that provide free ART to around 700.000 PLHIV. But again, at the micro level, many PLHIV prefer to keep their status to themselves: they have faced and still do face discrimination from relatives and friends.
In fact, I would think of the ART as one of the five central areas in which we have met with success in the last 28 years:
Counselling is a central component of HIV/AIDS initiatives. There is pre-test counselling before the HIV testing, then post-test counselling for persons whose HIV testing is negative but who practice risk behaviour, post-test counselling for those who are detected positive for the first time. There is also supportive counselling, nutritional counselling, counselling for ART, counselling for adherence, follow-up counselling, family counselling, bereavement counselling, counselling for PMTCT, counselling for children. Counselling is thus the process that links up prevention, care and support. ART itself requires counselling, since the therapy will have to be followed for the rest of the PLHIV’s life. Counselling has shown tremendous results: it helps the acceptance process for individuals and for families. Children living with HIV (CLHIV) were really the missing face of HIV. Most of the children below 15 years who are HIV-positive have acquired it from their mothers during the pregnancy. The issues of when to tell a child, what and how to tell her are always challenging. ART for children needs to be in smaller doses and sometimes in syrup form. These were not available earlier, and we had to powder or break adult tablets and give them. These issues were challenges over the years, but they are now slowly being resolved. Also, among our CLHIV we have about 30 children who are orphans, and they live with extended family. HIV/AIDS is a dynamic field, and we have to keep moving with the times, and evolve so that we can offer the best under changing circumstances. Recently, ASHA, in partnership with YRG Care, Chennai and Seriousfun, USA, has started a new endeavour: Camp Rainbow. We take CLHIV to a summer camp and use the opportunity to tell them all about HIV through games, stories and fun activities. We now have CLHIV who are in their late teens and early twenties and we discuss career options, marriage issues, etc. with them.  Finding new ways to work with CLHIV: Camp Rainbow
Women in prostitution, men who have sex with men, injecting drug users and transgender form what is known as groups practicing risk behaviour. In these groups, the prevalence of HIV infection varies from 2.5 % to 7%, vis-à-vis 0.35% in the general community. The link between these two sections of the communities is the ‘bridge population’, which includes truck drivers and migrants.
The risk groups face considerable S&D. For example, a woman in sex work who becomes HIV positive faces a triple stigma — she is HIV-positive, she is in sex work and she is a woman. The reason why they face so much S&D is cultural – because the kind of life they lead is considered taboo and unacceptable in Indian culture. This, in turn, leads to secrecy and inability to access services, both for prevention and care-support. As individuals, we may grow more accepting and non-judgemental, but at the policy level there are hindrances. Naturally, HIV/AIDS and sex, and sex culture, are linked. But indeed, even 28 years after of the entry of the epidemic into India, we as a nation still consider sex and sexuality to be a taboo topic. This does hamper prevention efforts, because of the sense of secrecy that grows around these issues. Government policies such as 377 can also impact prevention and treatment of HIV infection negatively, because the disease, then, tends to go underground in such instances and access becomes an issue. In the 1980s and 1990s, there was a real concern that India would be the next flashpoint for HIV/AIDS after Africa. Luckily, it did not happen. Our seroprevalence is low but the numbers are high, simply because the population itself is high. Thanks to the Government, NGOs, the civil society and positive networks, we are much better off than we thought we would ever be. But of course, we need to continue with all the efforts and not take HIV casually at any point in time. |
According to a recent UNAIDS report, India has the third highest number of HIV-positive people in the world. If, as a nation, we continue discriminating on the basis of caste, would it really surprise anyone if those suffering from HIV or AIDS also receive unfair treatments? Officially, efforts are made to improve this status quo. In February 2014, an HIV Bill was tabled before the Rajya Sabha, but unfortunately, it was subsequently withdrawn. The Bill sought to prohibit any kind of discrimination against infected individuals. The General Elections have seen mastery in political communication. But now, political leadership that goes beyond vote bank politics is the need of the hour. We may need to look at other parts of the world for some inspiration. I recall how, in November 2003, Festus Mogae, the President of Botswana, appeared on BBC with a journalist in an hour-long programme. He had accepted to receive questions from a worldwide audience in relation to the crisis the disease had caused in his country, with one third of its population HIV-positive.  Festus Mogae has set the level
in terms of political engagement on AIDS Governments routinely come in for criticism in the way they handle AIDS, especially in those countries where it has not been brought under control. Often enough, such criticism is justified. The President’s decision to come on camera was a brave one; and a measure of his openness to hear criticism and views on how the crisis should be handled. He did attempt to clarify to his audience, more than once, that he was not ‘the enemy’. “Tell me what to do”, he seemed to be saying, “and I will do it. I want to bring this disease under control.” Mogae was eager to do more than political communication: he tried being a model. He got himself tested, and publicly encouraged his ministers to take the test. He tried, thus, to emphasise the importance of being clear on one’s HIV status – whether one has participated in unsafe sex practices, or has reasons to suspect of having been exposed to the virus. After resigning in 2008, Festus Mogae joined in 2010 the advisory board of TeachAIDS, a Californian organization designing prevention material used over thirty countries.
Law, and, with the example of Mogae, politics, can be the fields in which HIV/AIDS discrimination is combated. But, when politics fails to do the necessary, we still have another path: culture. In 2004-2005, I decided to write a play on HIV/AIDS: High Fidelity Transmission. I opted for a play rather than a novel with the view of making it participatory. An NGO in Rajasthan used it to conduct workshops. A play permits this exercise in empathy by a community. Individuals can enact characters and explore the problems at hand more deeply, more personally. A novel may not have allowed this direct a use.  Theatre can be a powerful way to spread the word on AIDS.
Here, in South Africa A word about the title of the play. ‘High Fidelity Transmission’ is a play on the expression ‘high fidelity.’ One of the central characters in my play contracts HIV through a single unprotected sexual encounter. While I was completing the play, in end July 2004, there was a global conference on AIDS at Bangkok. One of the issues raised there by some groups was the mistaken emphasis the United States Government was placing on abstinence instead of promoting condom use as the actual weapon to combat the spread of AIDS. It was being pointed out by activist women from Africa how abstinence was no solution for married women, who might contract the disease from their husbands. The title of the play came to my mind in this context: marital infidelity is not the root of HIV dissemination. But this confusion also concerns us in India. Christians are a minority in our country and yet, the Church has conducted useful and charitable work connected with AIDS for decades now. I would not target them as such, but the attitude of the Catholic Church towards condoms is indefensible. In my play, the character of the nun who distributes condoms is based on a real life character. On the ground, workers sometimes understand reality better. It is also not a coincidence that Ulfat, the college lecturer, contracts AIDS after a single unprotected sexual encounter as does Raju. The far more promiscuous Hoover escapes unscathed – but he uses protections.
While writing a play on AIDS, it is difficult not to be concerned about promoting awareness related to the disease. There is always a social concern, beyond the creative effort. But at the same time, if there is too much information in the play, it may make for a dull, uninteresting viewing. Then, the whole point is lost and an information booklet format may have been more appropriate. In fact, this is one of the frequent and valid criticisms worded towards governments in the context of AIDS prevention: they handle their literacy campaigns in a dull, unimaginative fashion. Perhaps because of a lack of incentives, many government servants may not have the commitment necessary to tackle this kind of complex issue with creativity and effectiveness. In this context, individual initiatives can make a difference. I do not have a medical background and am certainly no expert on AIDS in its social and other manifestations. However, for a period of time, I was closely associated with a group of individuals in New Delhi whose campaigns focused on ending discriminatory treatment of individuals infected with the disease. The AIDS Bhedbhav Virodhi Andolan (AIDS Anti-Discrimination Movement) consisted of a number of completely unpaid volunteers. Among the group members there was a nun, a qualified doctor and former Registrar from the Maulana Azad Medical Center, a gynecologist, a professional blood donor, and other concerned citizens. The group released important reports, connecting AIDS in particular with the condition of women, with drug problems in the North East, and other such connected situations. All these reports were published without any funding, through individual contributions. My work with the group helped sensitise me to many connected issues, such as the cultural climate of homosexuality, and the community of the hijras in the sub continent. I would later dedicate several works to these topics: respectively, my play Inside Gayland and a study, The Third Sex and Human Rights. 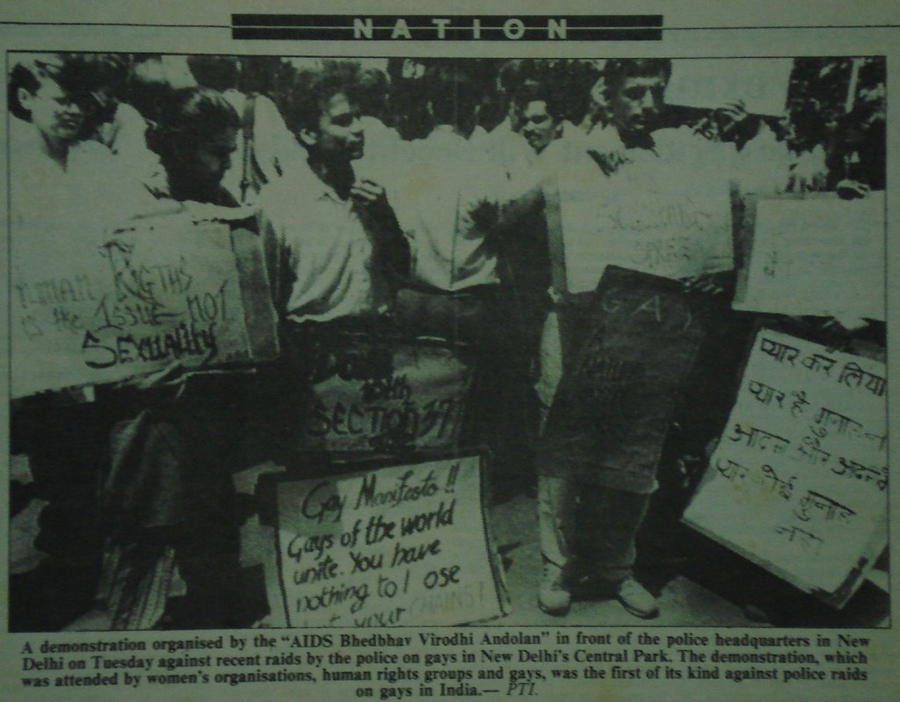 ABVA in 1992
Through High Fidelity Transmission, I tried addressing some of the other problems of AIDS prevention in India. The large funding received by organisations in the name of AIDS, and the little output they produce for the money, is one of them. In contrast, the dedication of small groups working against the disease without any remuneration whatsoever is striking. As a lawyer on behalf of the ABVA, I filed a petition challenging a purported action by the Tihar jail administration, to conduct mandatory HIV testing inside the prison. When the petition finally came up for hearing, the jail administration was taken aback by the position taken by the medical establishment, a pro-forma party in the case, who agreed with us that as per WHO guidelines, mandatory testing only succeeds in driving the disease underground. It had needed the initiative of a small group to take up the case. Ways must be found to make individual initiatives and the efforts of small groups merge with the institutional campaigns of bigger actors. |
||||||||
|
Glory Alexander is the founder of ASHA Foundation, Bangalore. A Charitable Trust, ASHA was started in 1998, and it works in the field of HIV/AIDS and provides awareness, testing and counseling services, medical care and treatment, rehabilitation, empowerment of women, adolescent health education, prevention of mother to child transmission of HIV services, and capacity building. Glory Alexander is a medical doctor, and she did her graduate and post-graduate in Internal Medicine from Christian Medical College and Hospital, Vellore.
|
Rajesh Talwar is currently working in the Department of Peacekeeping (DPKO) for the United Nations Assistance Mission in Afghanistan (UNAMA). He is a lawyer by profession, after studies in Negotiation at Harvard, Human Rights Law at Nottingham, and Law and Economics at Delhi University. He has taught law at Delhi University and Jamia Milia Islamia. Rajesh Talwar has worked for the United Nations on legal and justice-related issues in Somalia, Liberia, Kosovo, Afghanistan and Timor-Leste. He is the author of more than a dozen books, of which the most recent is Courting Injusice: The Nirbhaya Case and Its Aftermath (Hay House, 2013). Many of them, including High Fidelity Transmission, are available here.
|
||||||||



Disclaimers: The opinions expressed by the writers are their own. They do not represent their institutions’ view.
LILA Inter-actions will not be responsible for the views presented.
The images and the videos used are only intended to provide multiple perspectives on the fields under discussion.
Images and videos courtesy: Howal Miller | Earth Times | IBN Live | Woman’s Organisation in Rural Development | NGO Pulse | Women News Network | Orinam
Voice courtesy: Samuel Buchoul
Share this debate… |
… follow LILA… |
||||
  |
  |
  |
|||